

By: Juan Manuel Orjuela, MD
Neuropsychiatrist
Medicinal cannabis and dementia
The use of medicinal cannabis to treat neurodegenerative diseases has increased in recent years. Preclinical studies have documented cannabidiol (CBD) and tetrahydrocannabinol’s (THC) neuroprotective effects in mice and cell tissues. Similarly, research involving human subjects has also explored their potential to help manage psychological and behavioral symptoms such as anxiety, agitation, and aggression, within the context of Alzheimer’s disease and other dementias.
Dementia refers to a person who experience cognitive impairment including memory, attention, and language, often associated with advanced age. The individual’s capabilities decline gradually, leading to a loss of independence in activities such as cooking, driving, or managing finances. The term “dementia” has become outdated; in neuropsychiatry it is now known as major neurocognitive disorder. Among these, Alzheimer’s disease is the most prevalent, with 60-70% of all cases.
The prevalence of Alzheimer’s disease has been increasing steadily as the world population ages and diagnostic methods improve. According to the World Health Organization (WHO), over 50 million people worldwide live with dementia, primarily as a consequence of Alzheimer’s disease. Without effective treatments, this number is projected to triple by 2050, impacting more than 152 million people.
Alzheimer’s disease not only affects the individuals diagnosed, but also their families and caregivers. As the condition progresses, patients require more specialized care, leading to significant emotional and financial burden for their support networks. Moreover, Alzheimer’s has considerable economic implications for healthcare systems due to the substantial cost of care and treatment.

Some preclinical research has documented that using certain cannabinoids, such as CBD and THC (at low doses) may be effective at reducing neurodegeneration. This occurs because the central nervous system has, in addition to neurons, glial cells such as astrocytes and microglia. The latter have type-2 cannabinoid receptors (CB2R). Stimulation of these receptors have been shown to reduce inflammatory responses and enhance the degradation of abnormal proteins including beta-amyloid. . This is significant because the accumulation of beta-amyloid and the formation of related plaques are key features of Alzheimer’s disease. Though this is not proof that the disease is stopped or reversed, but it does initiate an avenue of exploration into the possibility of replicating these effects in humans and potentially modifying the course of the disease.
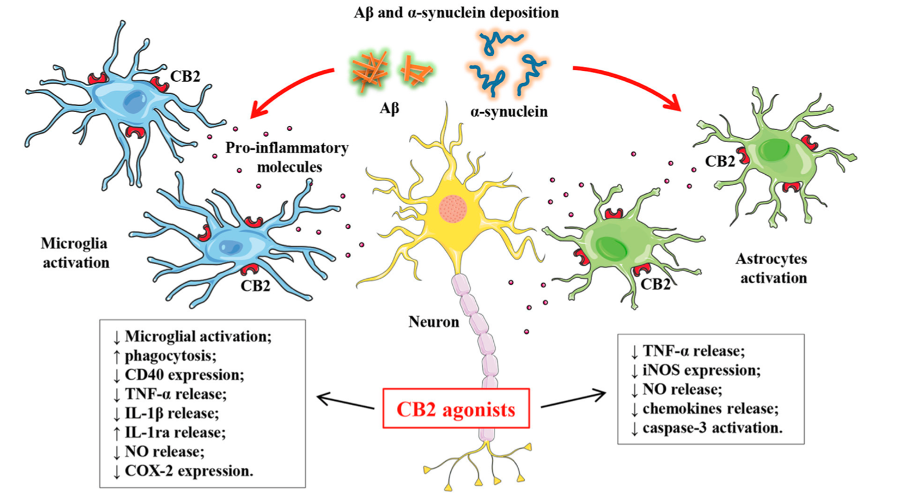
Source: Cassano T. Cannabinoid Receptor 2 Signaling in Neurodegenerative Disorders: From Pathogenesis to a Promising Therapeutic Target. 2017. Frontiers in Neuroscience
It has also been documented that CBD and THC can reduce neurotoxic effects and neuronal death by protecting cells from glutamate overstimulation. The inflammatory process in neurodegenerative diseases generates excess glutamate, an excitatory neurotransmitter, which promotes the entry of calcium into neurons and ultimately activates cell death mechanisms. Type-1 cannabinoid receptors (CB1R), when activated by THC or endocannabinoids such as anandamide, reduce calcium entry and protect neuron vitality.
Similarly, some clinical research shows that CBD and low doses of THC (less than 10 mg/day), administered together as an oral oil, reduce symptoms of agitation, anxiety, and aggression in people with dementia. Therefore, cannabinoids may have the potential to treat these neuropsychiatric symptoms without undesirable side effects such as sedation, dizziness, and gait instability, often linked to mainstream antipsychotic, anxiolytic, and antidepressant, treatments commonly used to manage these symptoms. This could improve patient and caregiver’s quality of life by providing a safe and effective treatment for common neuropsychiatric symptoms of Alzheimer’s Disease.

The mechanisms by which cannabinoids might reduce symptoms of agitation in people with dementia are not fully understood. However, it is known that in Alzheimer’s disease the endocannabinoid system is altered and brain regions such as the amygdala and hippocampus are deteriorated. These regions are responsible for emotional control and impulse regulation. Therefore, cannabinoids have the potential to modulate the disrupted endocannabinoid system w regions and provide symptomatic relief.
It is very important that patients and their families consult a doctor trained in medicinal cannabis prescription because cannabinoid treatment can have drug interactions, contraindications, and/or adverse effects. It is essential for the physician to evaluate whether medicinal cannabis is appropriate for the patient according to their profile and to start with low doses. Self-medication is not recommended for this type of treatment.
- Cassano, T., Calcagnini, S., Pace, L., De Marco, F., Romano, A., & Gaetani, S. (2017). Cannabinoid Receptor 2 Signaling in Neurodegenerative Disorders: From Pathogenesis to a Promising Therapeutic Target. Frontiers in neuroscience, 11, 30. https://doi.org/10.3389/fnins.2017.00030
- Woodward, M. R., Harper, D. G., Stolyar, A., Forester, B. P., & Ellison, J. M. (2014). Dronabinol for the Treatment of Agitation and Aggressive Behavior in Acutely Hospitalized Severely Demented Patients with Noncognitive Behavioral Symptoms. The American Journal of Geriatric Psychiatry, 22(4), 415–419. https://doi.org/10.1016/j.jagp.2012.11.022.
- Cao, C., Li, Y., Liu, H., Bai, G., Mayl, J., Lin, X., Sutherland, K., Nabar, N., & Cai, J. (2014). The Potential Therapeutic Effects of THC on Alzheimer’s Disease. Journal of Alzheimer’s Disease, 42(3), 973–984. https://doi.org/10.3233/JAD-140093.
- Alexandri, F., Papadopoulou, L., Tsolaki, A., Papantoniou, G., Athanasiadis, L., & Tsolaki, M. (2023). The Effect of Cannabidiol 3% on Neuropsychiatric Symptoms in Dementia – Six-Month Follow-Up. Clinical gerontologist, 1–8. Advance online publication. https://doi.org/10.1080/07317115.2023.2209563



